Post-Operative Analgesics
Two experts who are also clinicians compared the benefit-safety balance of eight post-operative analgesics on three favourable effects:
They also considered 14 unfavourable effects: six adverse events and eight serious adverse events (listed in the table at the bottom of this page).
- Pain relief
- Duration of action
- Opioid sparing
They also considered 14 unfavourable effects: six adverse events and eight serious adverse events (listed in the table at the bottom of this page).
The options
The total benefit-safety balance is shown here on a 100-point scale. Green best; Red worst. (Doses as indicated for post-operative pain control; morphine considered as 4mg.)
The total benefit-safety balance is shown here on a 100-point scale. Green best; Red worst. (Doses as indicated for post-operative pain control; morphine considered as 4mg.)
- Parecoxib 93
- Diclofenac 80
- Keterolac 75
- Metamizol 74
- Nefopam 68
- Acetaminophen 66
- Tramadol 60
- Morphine 57
- Placebo 36
The numbers represent the overall added clinical value of each analgesic. They take into account available data for the effects and judgements by the experts about the clinical relevance of the effects.
After the favourable effects have been weighted for their added clinical value, they are described as benefits. For the unfavourable effects, the inverse of their weighted loss-of-value is referred to as safety. The assessments do not consider contra-indications, interactions with any drugs, or any precautions.
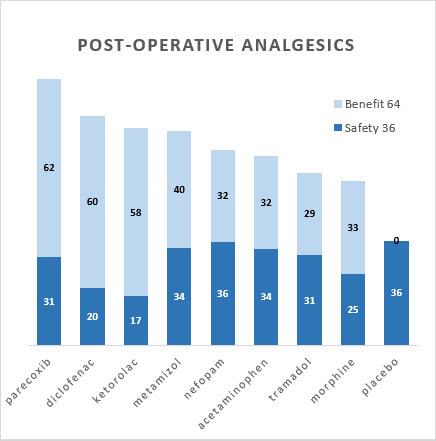
Bar graphs
Separate contributions of benefits and safety to the totals show different profiles. For example, ketorolac and metamizol score similarly overall, but keterolac is better in benefits while metamizol is safer.
Separate contributions of benefits and safety to the totals show different profiles. For example, ketorolac and metamizol score similarly overall, but keterolac is better in benefits while metamizol is safer.
Benefits versus Safety
Another way to look at the benefit and safety information is to show each drug's two assessments before the 64-36 weights are applied.
Another way to look at the benefit and safety information is to show each drug's two assessments before the 64-36 weights are applied.
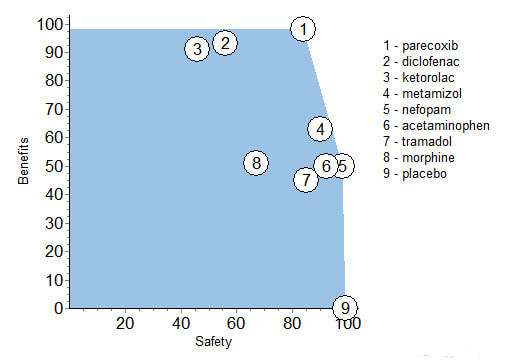
Note that parecoxib is better than morphine in both benefits and safety. Tramadol is about as safe as parecocib, but the latter is more beneficial. Also, nefopam is better in both benefits and safety than tramadol, and is about the same in benefits as acetaminophen, but is safer. These dominance relationships suggest that overall, parecoxib or nefopam are better than any of the other analgesics in benefits, or in safety, or both benefits and safety.
Effects Table
All the above is based on the following data, culled from available public sources, and experts' weight assessments about the clinical relevance of the evidence.
For the Duration of Action and Opioid Sparing, the figures are medians of data gleaned from published data. For the remaining unfavourable effects, data were limited or not available, so the experts discussed available published research and shared their experience and knowledge in assessing direct preference values ranging from zero to 100.
To support patient-oriented prescribing based on the evidence, green shading identifies the best drug for each favourable effect with red the worst drug for each unfavourable effect.
All the above is based on the following data, culled from available public sources, and experts' weight assessments about the clinical relevance of the evidence.
For the Duration of Action and Opioid Sparing, the figures are medians of data gleaned from published data. For the remaining unfavourable effects, data were limited or not available, so the experts discussed available published research and shared their experience and knowledge in assessing direct preference values ranging from zero to 100.
To support patient-oriented prescribing based on the evidence, green shading identifies the best drug for each favourable effect with red the worst drug for each unfavourable effect.
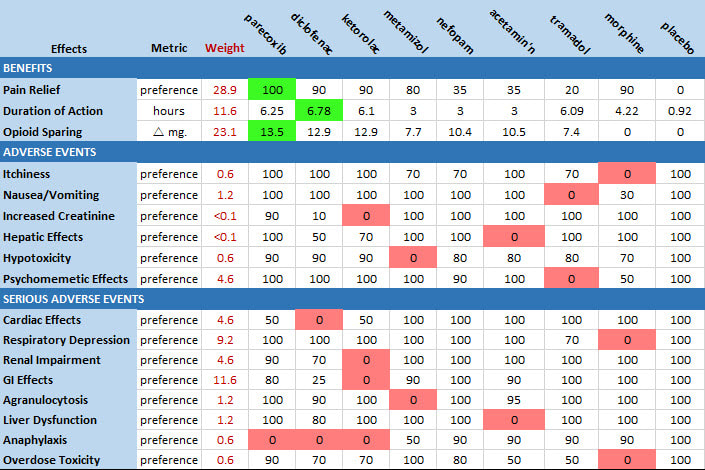
Pain relief: Proportion of patients reporting at least 50% pain relief within 4 hours.
Duration of action: Median time to rescue medication.
Opioid sparing: Mean reduction in mg. of 24hr morphine consumption.
Duration of action: Median time to rescue medication.
Opioid sparing: Mean reduction in mg. of 24hr morphine consumption.
Note that the weighted scores are relative and zero does not mean no value, so only differences between numbers, not their ratios, make sense for comparing the clinical value they represent.
The MCDA model was created over five workshops with Pfizer specialists who agreed the analgesics to be compared and the favourable and unfavourable effects, followed by a decision conference in which the two clinicians/experts validated the model and applied their clinical judgement. The main limitation of this analysis is that the preference values and weights are based mainly on the judgements of only two independent experts/clinicians.
Source: Schug, S., Pogatzki-Zahn, E., Phillips, L. D., Essex, M. N., Xia, F., Reader, A. J., & Pawinski, R. (2020). Multi-Criteria Decision Analysis to Develop an Efficacy-Safety Profile of Parenteral Analgesics Used in the Treatment of Postoperative Pain. Journal of Pain Research, 13, 1969-1977.
Source: Schug, S., Pogatzki-Zahn, E., Phillips, L. D., Essex, M. N., Xia, F., Reader, A. J., & Pawinski, R. (2020). Multi-Criteria Decision Analysis to Develop an Efficacy-Safety Profile of Parenteral Analgesics Used in the Treatment of Postoperative Pain. Journal of Pain Research, 13, 1969-1977.